

Maurice Termeer, Javier Oliván Bescós, Marcel Breeuwer, Anna Vilanova i Bartroli , Frans Gerritsen, Eduard Gröller, Eike Nagel
, Frans Gerritsen, Eduard Gröller, Eike Nagel
Patient-Specific Coronary Artery Supply Territory AHA Diagrams
Poster shown at SCMR 2009
(29. January 2009- 1. February 2009)
In Abstracts of the 12th Annual SCMR Scientific Sessions - 2009
, pages 164-165.
[ abstract] [
abstract] [ poster]
poster]
Information
- Publication Type: Poster
- Workgroup(s)/Project(s):
- Date: January 2009
- Journal: Journal of Cardiovascular Magnetic Resonance
- Volume: 11
- Series: 1
- Location: Orlando, Florida
- ISSN: 1532-429X
- Event: SCMR 2009
- Booktitle: Abstracts of the 12th Annual SCMR Scientific Sessions - 2009
- Conference date: 29. January 2009 – 1. February 2009
- Pages: 164 – 165
- Keywords: coronary supply territories, patient-specific bulls eye plot
Abstract
Introduction: The American Heart Association proposed a 17-segment model for the segmentation of the left ventricle together with a mapping from each segment to a supplying coronary artery. This proposal is based on population averages. Several studies have confirmed the inaccuracy of this mapping due to large anatomical variations of the coronary arteries among individuals. Several proposals have been made for a different mapping between the 17 segments and the coronary arteries.Purpose: Due to the large variation in coronary anatomy there is a need for a patient-specific assignment of ventricular segments to supplying coronary arteries. We propose to use a segmentation of the coronary arteries and the ventricular epicardium to compute this patient-specific mapping.
Methods: The three primary coronary arteries (LAD, LCX and RCA) and the left ventricle are segmented in a whole-heart MRI (SSFP) or CT scan of at least 150 slices. For the coronary arteries we employ a semi-automatic vessel tracking algorithm. The left ventricle is segmented using a fully automatic approach. The epicardial surface of the resulting segmentation is represented as a quadrilateral mesh. The centerlines of the coronary arteries are projected on the epicardial surface. A Voronoi diagram of the projected arteries is computed using a geodesic distance metric. The patient-specific coronary supply territories are computed using a modified marching squares algorithm. The examples given here consist of three territories, but our approach is flexible enough to handle any amount of territories.
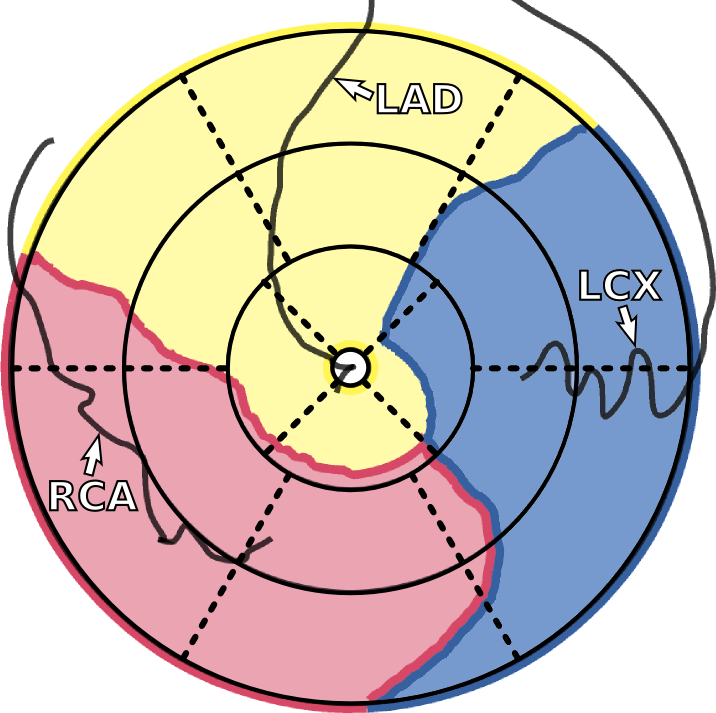
Both the coronary supply territories and the coronary arteries are projected onto a bull’s eye plot using a parameterization of the left ventricle based on cylindrical coordinates, using the cardiac long axis as the primary axis of the cylinder (Figure 1a). The continuous nature of the epicardial surface is preserved in this projection. This means that the bull’s eye plot does not consist of rings representing slices, but that the distance to the center is proportional to the distance to the apex. This bull’s eye plot can for example be used as an overlay for the analysis of viability (Figure 1b).
Figure 1. (a) Bull’s eye plot showing patient-specific coronary supply territories. The dotted lines represent the 17-segment model. (b) Patient-specific coronary supply territories as an overlay on a bull’s eye plot of a late enhancement scan.
Results: We evaluated our method on image data from five patients. For each patient we produced both a standard 17-segment diagram and a diagram with the projection of the patient-specific coronary supply territories resulting from our approach. In both diagrams a projection of the segmented coronary arteries was shown. We then asked an experienced clinician to judge the correspondence between the coronary arteries and the suggested coronary supply territories for both diagrams. It was judged that our patient-specific coronary supply territories provide a better correlation with the position of the coronary arteries. The clinician expressed a preference to our method as compared to the standard 17-segment model.
The continuous relation between the distance to the center of the bull’s eye plot and the distance to the apex caused some confusion with our clinician. Especially in combination with CMR data consisting of relatively few slices this relation should be clarified.
Conclusion: With our method the relation between coronary arteries and areas supplied by these arteries is better visualized. This will help to better correlate the location of infarcted or ischemic areas to the coronaries that have caused the respective infarction or ischemia.
Additional Files and Images


Weblinks
No further information available.BibTeX
@misc{termeer-2009-scmr,
title = "Patient-Specific Coronary Artery Supply Territory AHA
Diagrams",
author = "Maurice Termeer and Javier Oliv\'{a}n Besc\'{o}s and Marcel
Breeuwer and Anna Vilanova i Bartroli and Frans Gerritsen
and Eduard Gr\"{o}ller and Eike Nagel",
year = "2009",
abstract = "Introduction: The American Heart Association proposed a
17-segment model for the segmentation of the left ventricle
together with a mapping from each segment to a supplying
coronary artery. This proposal is based on population
averages. Several studies have confirmed the inaccuracy of
this mapping due to large anatomical variations of the
coronary arteries among individuals. Several proposals have
been made for a different mapping between the 17 segments
and the coronary arteries. Purpose: Due to the large
variation in coronary anatomy there is a need for a
patient-specific assignment of ventricular segments to
supplying coronary arteries. We propose to use a
segmentation of the coronary arteries and the ventricular
epicardium to compute this patient-specific mapping.
Methods: The three primary coronary arteries (LAD, LCX and
RCA) and the left ventricle are segmented in a whole-heart
MRI (SSFP) or CT scan of at least 150 slices. For the
coronary arteries we employ a semi-automatic vessel tracking
algorithm. The left ventricle is segmented using a fully
automatic approach. The epicardial surface of the resulting
segmentation is represented as a quadrilateral mesh. The
centerlines of the coronary arteries are projected on the
epicardial surface. A Voronoi diagram of the projected
arteries is computed using a geodesic distance metric. The
patient-specific coronary supply territories are computed
using a modified marching squares algorithm. The examples
given here consist of three territories, but our approach is
flexible enough to handle any amount of territories. Both
the coronary supply territories and the coronary arteries
are projected onto a bull’s eye plot using a
parameterization of the left ventricle based on cylindrical
coordinates, using the cardiac long axis as the primary axis
of the cylinder (Figure 1a). The continuous nature of the
epicardial surface is preserved in this projection. This
means that the bull’s eye plot does not consist of rings
representing slices, but that the distance to the center is
proportional to the distance to the apex. This bull’s eye
plot can for example be used as an overlay for the analysis
of viability (Figure 1b). Figure 1. (a) Bull’s eye plot
showing patient-specific coronary supply territories. The
dotted lines represent the 17-segment model. (b)
Patient-specific coronary supply territories as an overlay
on a bull’s eye plot of a late enhancement scan. Results:
We evaluated our method on image data from five patients.
For each patient we produced both a standard 17-segment
diagram and a diagram with the projection of the
patient-specific coronary supply territories resulting from
our approach. In both diagrams a projection of the segmented
coronary arteries was shown. We then asked an experienced
clinician to judge the correspondence between the coronary
arteries and the suggested coronary supply territories for
both diagrams. It was judged that our patient-specific
coronary supply territories provide a better correlation
with the position of the coronary arteries. The clinician
expressed a preference to our method as compared to the
standard 17-segment model. The continuous relation between
the distance to the center of the bull’s eye plot and the
distance to the apex caused some confusion with our
clinician. Especially in combination with CMR data
consisting of relatively few slices this relation should be
clarified. Conclusion: With our method the relation between
coronary arteries and areas supplied by these arteries is
better visualized. This will help to better correlate the
location of infarcted or ischemic areas to the coronaries
that have caused the respective infarction or ischemia.",
month = jan,
journal = "Journal of Cardiovascular Magnetic Resonance",
volume = "11",
series = "1",
location = "Orlando, Florida",
issn = "1532-429X ",
event = "SCMR 2009",
booktitle = "Abstracts of the 12th Annual SCMR Scientific Sessions - 2009",
Conference date = "Poster presented at SCMR 2009 (2009-01-29--2009-02-01)",
note = "164--165",
pages = "164 – 165",
keywords = "coronary supply territories, patient-specific bulls eye plot",
URL = "https://www.cg.tuwien.ac.at/research/publications/2009/termeer-2009-scmr/",
}